Tamil Nadu is a state in southern India with more than 80 million residents, about the same population as Germany. When the coronavirus pandemic struck earlier this year, the state faced enormous challenges, ranging from answering citizens’ questions about COVID-19 to identifying people who needed urgent care. As rules around the nationwide lockdown were gradually relaxed, Tamil Nadu also needed to ensure that information was communicated to those who needed it.
Santosh Misra, CEO of the Tamil Nadu e-Governance Agency (TNeGA), was tasked with developing and driving technology-related initiatives to tackle these problems and more for Tamil Nadu. In this interview, he speaks with Wharton marketing professor Raghuram Iyengar, faculty director of Wharton Customer Analytics, about the role that TNeGA played in e-governance for the state and the initiatives the agency deployed to contain the crisis.
Raghuram Iyengar: Thank you for taking the time during the crisis for this interview. Can you give our readers a brief description of your background?
Santosh Misra: I would describe myself as a public policy specialist working in emerging technologies for improved governance and service delivery to citizens. I have a strong technology background with more than 20 years of experience in information technology and public policy. I have a bachelor’s degree in electrical engineering from the Indian Institute of Technology, Kanpur, and a master’s degree in electrical engineering from the University of Minnesota.
After working for a few years at Bell Labs, I decided to apply for the Indian Administrative Service (IAS), India’s premier civil service. It was a highly unusual career shift from the cutting edge of technological environs of Bell Labs to the deep rural hinterlands of India. It was also not an easy decision to leave a well settled (financially as well as professionally) career. But I was convinced that I wanted to work at the grass roots level in my country and be connected directly to the people.
Iyengar: What is your current role in the Tamil Nadu state government?
Misra: I am the CEO of the Tamil Nadu e-Governance Agency (TNeGA). We run the e-Sevai (sevai means “service” in the Tamil language) technology platform to offer some 150 government services (e.g., social security application, land records) to citizens. We manage a network of approximately 12,000 e-Sevai centers spread all over the state, which process more than 10 million individual service requests each year.
.Iyengar: Can you describe the mandate of the e-governance agency and give some examples of what projects the agency has been involved with in the past?
Misra: I lead programs that require a strategic change within the Tamil Nadu government using technology. Some policies that I take pride in having a major role in conceptualizing for the state government are in the areas of artificial intelligence, blockchain, digital identity, and vocational education. Specifically, the Tamil Nadu e-governance Agency has been involved in:
- State-wide blockchain backbone: This would be the largest government-led deployment of blockchain anywhere in the world, with almost the entire population of the state connected through it. The goal is to have the blockchain serve as a privacy protecting, secure and trusted platform for the government to exchange information with citizens.
- Predictive analytics for public services: This project aims to revolutionize the way government services are delivered to citizens. This initiative coupled with a blockchain enabled digital wallet for every citizen will be a game changer for public service delivery.
- AI for good: We have initiated several projects in the areas of education, health care, and agriculture. These involve artificial intelligence (AI) and the Internet of Things (IoT). A few of them are:
- Facial recognition systems in schools for monitoring attendance.
- AI-based pest and disease identification in crops.
- IoT-based monitoring of drinking water supply in rural areas.
Iyengar: Given the current crisis surrounding the coronavirus, how is the e-governance agency involved in dealing with its different aspects?
Misra: The coronavirus crisis came as a big shock especially in terms of its scale and impact. A country of almost 1.3 billion people went under a lockdown. The whole economy came to a grinding halt. The state of Tamil Nadu suffered the same fate. To understand the scale, the state has 80 million people and is home to more than 300,000 small, medium-sized and large enterprises. In addition, the population of migrant workers (from other parts of the country) is about 2 million or so.
When the wheels of the economy stop churning and state borders start getting sealed, it is an enormous challenge to coordinate the unrestricted movement of emergency personnel and essential goods (e.g., pharmaceuticals, food and agricultural products). There is a need for real time information from the field, hospitals, Interactive Voice Response System (IVRS) helplines and testing labs for policy makers and the public health managers. Live status updates of containment zones, infection trends, heat maps and infection spread are needed as well. Finally, the government also requires a clear line of communication with its citizens.
My agency was responsible for providing most of the technology and the support around data analytics to the government. Our support includes — but is not limited to — a variety of initiatives. We oversee contact tracing and the quarantine management system, hospital infrastructure management, TN ePASS system for movement of people and movement of industrial workers, GIS support for managing containment zones and hot spots, Arogya Setu (a Government of India mobile app for contact tracing) IVRS automated voice calls, and data analytics and data visualization for policy making. I will highlight two of these initiatives to provide some understanding of the impact of our offerings.
Arogya Setu IVRS system:
The Government of India introduced the Arogya Setu (loosely translated as “bridge to health”) app, which is a great tool for answering common queries about the coronavirus. The app allows users to do a self-assessment and determine if she or he needs to be tested for COVID-19. Keeping the diversity of languages in India into account, the app is multilingual. However, its reach is limited to smartphone users. While India has about 1.3 billion mobile phones, only about 30% of these are smart phones. Thus, if we wish to be inclusive, it is critical for us to devise strategies that can accommodate the remaining 70% of non-smart phone users.
Our agency took up the challenge of enhancing the applicability of Arogya Setu. We created an IVRS version of the app. Our project is TNeGA’s first large-scale technology deployment in collaboration with the Tamil Nadu health department, IIT Chennai, Department of Telecom, Government of India and Bharat Sanchar Nigam Limited, the state-owned telecom company. We were involved at every stage of the implementation. We designed the questions and wrote an algorithm to analyze the health condition of an individual based on their response on the IVRS system. Importantly, the system does not require an internet connection and is available in Tamil.
Here is how it works: Anyone can give a missed call to 94999 12345 (i.e., call the number and cancel so there is no charge for the user). Figure 1 shows more information about what the system does.
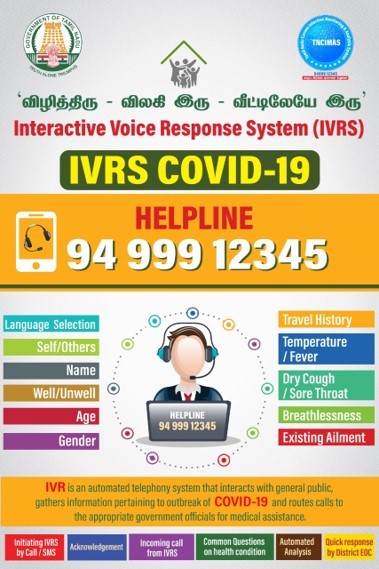
Figure 1: IVRS Helpline for COVID-19
Figure 2 below demonstrates the system’s call flow. The system calls the people back and asks them to respond to a set of simple questions about their age, health, and travel history. Their responses are analyzed and an infection risk categorization of the caller is done (red, yellow, or green). They are advised to follow standard protocols for isolation if needed and, in cases where there is a high risk of infection (the red category), the local district administration is notified.
We initiated the Arogya Setu IVRS on April 9. So far, we have received more than 150,000 calls. Of these calls, about 600 required immediate attention. The system has been enormously helpful in allocating medical resources to the right set of people.
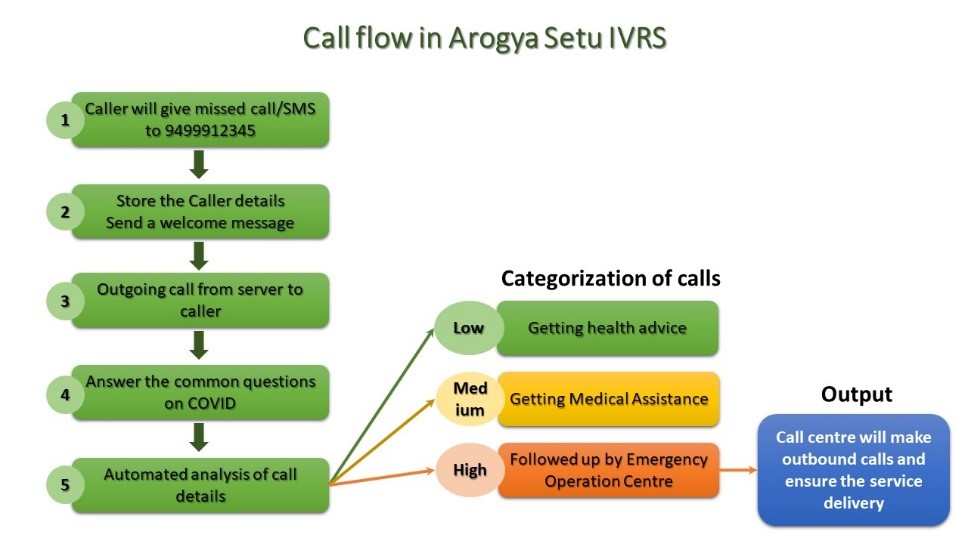
Figure 2: The call flow for IVRS Arogya Setu
TN ePASS system
The Government of Tamil Nadu, like other state governments in India, declared a state-wide lockdown and prohibited the non-essential movement of people. However, the movement of people providing essential services (e.g., health care, medicines, food etc.) had to keep running and people with personal emergencies also needed to move. To allow for regulated movement of people a system was needed, which would make the process easy and accessible to every citizen.
Our agency developed a unified movement portal called TN ePASS (https://tnepass.tnega.org ) to meet these needs. The Government of Tamil Nadu (following the guidelines of Government of India), partially relaxed the lockdown on May 3 and allowed certain industries to function at limited capacity. The portal was launched on May 2 to start providing passes for movement. People could use any smartphone, tablet, iPad, or laptop to apply for the passes. Those who found it difficult to access the Internet could use an e-Sevai center, which was designated as an ePASS help center.
These centers have been authorized to apply on behalf of people and provide their services free of charge. The ePASS application system is a set of two simple screens and it works with mobile number as login id (OTP-based access). Figure 3 below shows how the ePASS application is submitted.
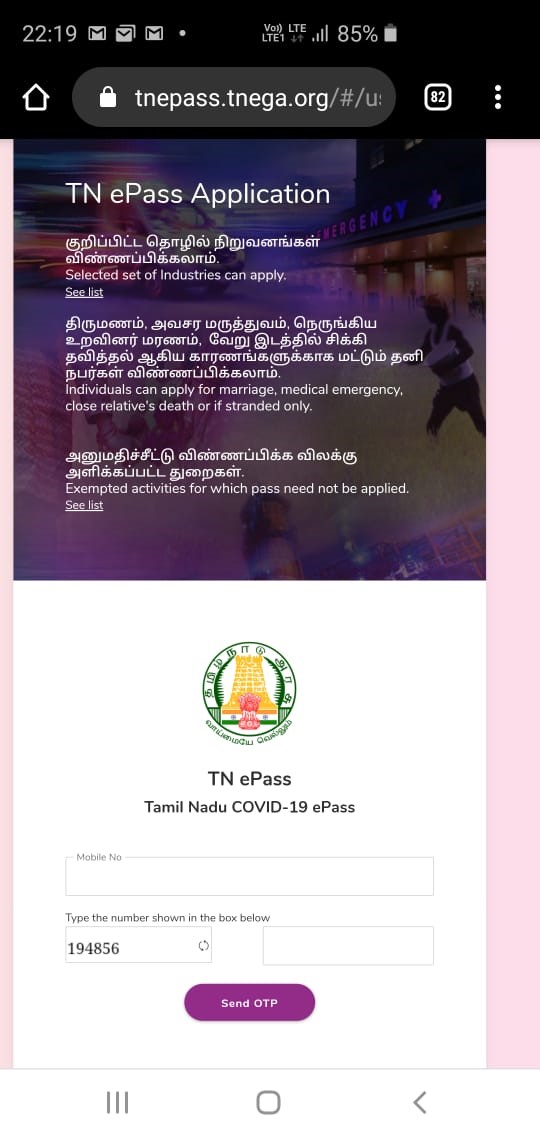
Figure 3: ePass application process
Here is how it works: The applicants get an SMS-based acknowledgement the moment they apply. Using their mobile number to log in (with a one-time password) on the TN ePASS website, they can see the status of their application. Once the pass is approved, another SMS is sent, and the applicant gets a short URL link to download the pass. The pass can also be downloaded on a laptop or any other internet-connected device, and it can also be obtained from e-Sevai centers. The TN ePass is a QR code enabled, color-coded pass which can be easily verified in the field by the police or other authorized officials for authenticity by using any commonly available QR code scanner apps for smartphones.
We have so far received more than 3.5 million applications for the ePass and successfully processed 3.45 million or so. The feedback for the system has been quite positive as it has helped in relatively seamless flow of emergency personnel.
Iyengar: What are some lessons from the initiatives during this crisis that can help us better prepare when the next crisis comes around?
Misra: For any strategic change to be implemented, it is important to keep the so-called C4s — Communication, Clarity (shared vision) and Champions of Change –- into account. Let me offer the examples of the two initiatives, ePass and Arogya Setu IVRS, to emphasize this point.
Both the ePass and Arogya Setu IVRS required large-scale collaboration across organizations in the private sector, public sector, academia, citizens and the government. Within the government as well, we needed support from different stakeholders – the police department, industries department, public department, and district collectors. For example, the TN ePASS system relied on the police for enforcement; on the industries department to plan phased unlocking of industries; the private sector for developing the highly dynamic platform; district collectors as the approving authority; and, above all, the citizens as users.
In any such complex multi-stakeholder technology initiative, the biggest challenge is that of effective and clear communication. The organizations need to have a shared vision (clarity) and be able to respond to unforeseen situations. The TN ePASS operates in a highly dynamic and constantly changing environment. Every week, a new regulation is introduced, or a new relaxation is announced. Apart from the solution delivery challenge, a significant challenge is being able to effectively communicate any change with all the key stakeholders.
Finally, we encouraged a change champion within each administrative and collaborative unit and provided active support to them to overcome any challenges. We created a WhatsApp group of key officials of each department who needed to respond in case any problems arose and who also gave us feedback from the field. This group helped develop a community of champions of change. That was critical in helping us with all aspects of implementation.
(Disclaimer: The opinions expressed above are Santosh Misra’s personal views and they do not represent the views of the Government of Tamil Nadu.)